:format(jpeg)/images/study_unit/the-oculomotor-trochlear-and-abducens-nerves/5JoLkkymfCjoMNx206eYw_Oculomotor__trochlear_and_abducens_nerves.png)
/images/vimeo_thumbnails/258819836/Vagj2qWn0uVhTyES1eQ_overlay.jpg)
:format(jpeg)/images/study_unit/the-oculomotor-trochlear-and-abducens-nerves/5JoLkkymfCjoMNx206eYw_Oculomotor__trochlear_and_abducens_nerves.png)
- Overview
- CN I:Olfactory Nerve
- CN II: Optic Nerve
- CN III: Oculomotor Nerve
- CN IV: Trochlear Nerve
- CN V: Trigeminal Nerve
- CN VI: Abducens Nerve
- CN VII: Facial Nerve
- CN VIII: Vestibulocochlear Nerve
- CN IX: Glossopharyngeal Nerve
- CN X: Vagus Nerve
- CN XI: Spinal Accessory Nerve
- CN XII: Hypoglossal Nerve
- Autonomic Innervation of the Head
-
Cranial nerves (CNN) emerge through openings in the skull and are covered by tubular sheaths of connective tissue derived from the cranial meninges.
There are 12 pairs of cranial nerves, numbered I to XII, from rostral to caudal.

Like spinal nerves, the 12 pairs of cranial nerves may possess one or a combination of the following sensory and motor modalities
-
- Sensory (afferent) neurons. Conduct information from the body tissues to the CNS.
- General sensory (general somatic afferent). Transmit sensory information (e.g., touch, pain, and temperature), conducted mainly by CN V but also by CNN VII, IX, and X.
- Special sensory (special visceral afferent). Include special sensory neurons (e.g., smell, vision, taste, hearing, and equilibrium), mainly conducted by the olfactory, optic, and vestibulocochlear nerves (CNN I, II, and VIII, respectively) as well as by CN VII and CN X.
- Visceral sensory (general visceral afferent). Convey sensory information from the viscera, including the gastrointestinal tract, trachea, bronchi, lungs, and heart, as well as the carotid body and sinus. Visceral sensory neurons course within CN IX and CN X.
- Motor (efferent) neurons. Conduct information from the CNS to body tissues.
- Somatic motor (general somatic efferent) neurons. Innervate skeletal muscles derived from somites, including the extraocular and tongue muscles. Innervation is accomplished via the oculomotor, trochlear, abducens, and hypoglossal nerves (CNN III, IV, VI, and XII, respectively).
- Branchial motor (special visceral efferent) neurons. Innervate skeletal muscles derived from the branchial arches, including the muscles of mastication and facial expression and the palatal, pharyngeal, laryngeal, trapezius and sternocleidomastoid muscles. Innervation is accomplished via the trigeminal, facial, glossopharyngeal, vagus, and spinal accessory nerves (CNN V, VII, IX, X, and XI, respectively).
- Visceral motor (general visceral efferent) neurons. Innervate involuntary (smooth) muscles or glands, including visceral motor neurons that constitute the cranial outflow of the parasympathetic division of the autonomic nervous system. The preganglionic neurons originate in the brainstem and synapse outside the brain in parasympathetic ganglia. The postganglionic neurons innervate smooth muscles and glands via CNN III, VII, IX, and X.

[Overview of the CNN.
Modalities of the Cranial NervesModality
General Function
CNN Containing the Modality
General sensory
Perception of touch, pain, temperature
CN V (trigeminal), CN VII (facial), CN IX (glossopharyngeal), CN X (vagus)
Special sensory
Vision, smell, hearing, balance, taste
CN I (olfactory), CN II (optic), CN VII (facial), CN IX (glossopharyngeal)
Visceral sensory
Sensory input from viscera
CN IX (glossopharyngeal), CN X (vagus)
Branchial motor
Motor innervation to skeletal muscle derived from branchial arches
CN V-3 (mandibular), CN VII (facial), CN IX (glossopharyngeal), CN X (vagus), CN XI (spinal accessory)
Somatic motor
Motor innervation of skeletal muscle derived from somites
CN III (oculomotor), CN IV (trochlear), CN VI (abducens), CN XII (hypoglossal)
Visceral motor
Motor innervation to smooth muscle, heart muscle, and glands
CN III (oculomotor), CN VII (facial), CN IX (glossopharyngeal), CN X (vagus)
]
The nuclei of the cranial nerves (where motor neurons originate or sensory neurons terminate) are located in the brainstem, with the exception of CN I and CN II, which are extensions of the forebrain.
Cranial Nerve Targets
The specific functions of cranial nerves depend on the nature of the anatomic targets of the cranial nerves
- CNN V, VII, IX, and X. Innervate almost all of the structures of the head and neck, such as the skin, mucous membranes, muscle, and glands derived from the pharyngeal arches. Of these four nerves, CN V and CN VII innervate most of these structures, whereas CN IX innervates only a few structures of the head, oral cavity, pharynx, and neck. Almost all targets of CN X are in the trunk.
- CNN III, IV, and VI. Innervate only structures in the orbit.
- CNN I, II, and VIII. Possess only special sensory neurons for smell, sight, balance, and hearing.
- CN XII. Innervates only the tongue muscles.
- CNN III, VII, IX, and X. The cranial nerves that carry parasympathetic neurons.
- Table 17-2. Overview of the Cranial Nerves
CN
Modalities and Function
Exit from Skull
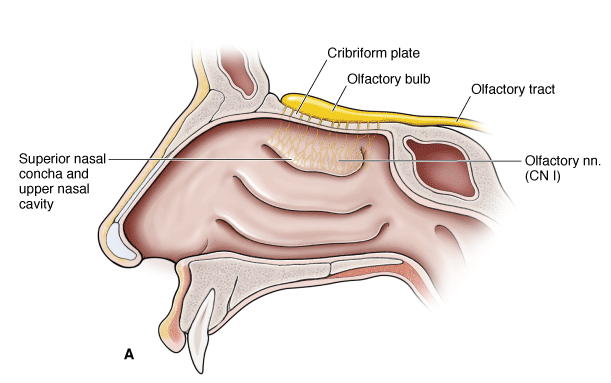
CN I (olfactory)
Special sensory: smell
Cribriform plate of the ethmoid bone
CN II (optic)
Special sensory: sight
Optic canal
CN III (oculomotor)
Somatic motor: levator palpebrae superioris m.; superior, medial, and inferior rectus mm.; inferior oblique mm.
Visceral motor: sphincter pupillae m. (pupil constriction) and ciliary mm. (lens accommodation)
Superior orbital fissure
CN IV (trochlear)
Somatic motor: superior oblique m.
Superior orbital fissure
CN V (trigeminal)
General sensory:
CN V-1: orbit and forehead
CN V-2: maxillary region
CN V-3: mandibular region, tongue
Branchial motor:
CN V-3: muscles of mastication, mylohyoid, anterior digastricus, tensor tympani, and tensor veli palatine mm.
CN V-1: superior orbital fissure
CN V-2: foramen rotundum
CN V-3: foramen ovale
CN VI (abducens)
Somatic motor: lateral rectus m.
Superior orbital fissure
CN VII (facial)
General sensory: external acoustic meatus and auricle
Special sensory: anterior two-thirds of tongue
Branchial motor: muscles of facial expression and stylohyoid, posterior digastricus, stapedius mm.
Visceral motor: all glands of the head (lacrimal, submandibular, sublingual, palatal, nasal) except the one it courses through (does not innervate the parotid)
Internal acoustic meatus
CN VIII (vestibulocochlear)
Special sensory: hearing, balance, and equilibrium
Internal acoustic meatus
CN IX (glossopharyngeal)
General sensory: posterior third of tongue, oropharynx, tympanic membrane, middle ear, and auditory tube
Special sensory: taste from posterior one-third of tongue
Visceral sensory: carotid sinus (baroreceptor) and carotid body (chemoreceptor)
Branchial motor: stylopharyngeus m.
Visceral motor: parotid gland
Jugular foramen
CN X (vagus)
General sensory: skin of the posterior ear and external acoustic meatus
Visceral sensory: aortic and carotid bodies (chemoreceptors) and aortic arch (baroreceptor)
Branchial motor: all palatal muscles (except tensor tympani); all pharyngeal muscles (except stylopharyngeus m.) and all laryngeal mm.
Visceral motor: heart, smooth muscle, and glands of the respiratory tract, gastrointestinal tube, and viscera of the foregut and midgut
Jugular foramen
CN XI (spinal accessory)
Branchial motor: trapezius and sternocleidomastoid mm.
Jugular foramen
CN XII (hypoglossal)
Somatic motor: tongue mm. (except palatoglossus m.)
Hypoglossal canal
- mm, muscles; m, muscle.
- Sensory (afferent) neurons. Conduct information from the body tissues to the CNS.
The optic nerve contains only special sensory neurons concerned with vision.
The optic nerve is a myelinated nerve conducting the retinal output to the central nervous system (CNS). It is composed of:
-
an intraocular portion, which is visible as the optic disk in the retina
-
an intraorbital portion
-
an intracanalicular portion
-
an intracranial portion
The nerve is ensheathed in meninges continuous with the brain.
At present, pharmacological treatment of optic neuropathies usually is based on management of the underlying disease. For example, nonarteritic ischemic optic neuropathy might be treated with intravitreal glucocorticoids (Kaderli et al., 2007) and optic neuritis may be best treated with intravenous glucocorticoids (Atkins et al., 2007; Beck and Gal, 2008; Volpe, 2008). Unfortunately, these guidelines have not yet become routine clinical practice (Biousse et al., 2009). Glaucomatous optic neuropathy is medically managed by decreasing IOP.
Pathways
Optic nerve fibers arise from the retina and all converge at the optic disc. The optic nerve emerges from the posterior surface of the globe through the posterior scleral foramen, a short, circular opening in the sclera about 1 mm below and 3 mm nasal to the posterior pole of the eye. The nerve fibers become myelinated on leaving the eye, increasing the diameter from 1.5 mm (within the sclera) to 3 mm (within the orbit). The orbital segment of the nerve is 25–30 mm long; it travels within the optic muscle cone, via the bony optic canal, and thus gains access to the cranial cavity. The intracanalicular portion measures 4–9 mm. After a 10 mm intracranial course, the nerve joins the opposite optic nerve to form the optic chiasm.
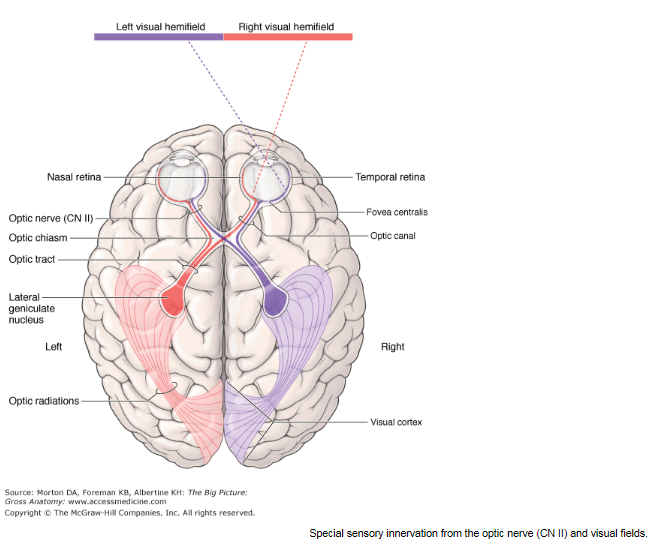
CN II exits the orbit via the optic canals. Both optic nerves form the optic chiasm, the site where neurons from the nasal side of either retina cross over to the contralateral side of the brain. The neurons then pass via the optic tracts to the thalamus, where they synapse with neurons that course to the primary visual cortex of the occipital lobe.
- Visual fields. The visual field is the part of the world seen by the eyes. The entire visual field is divided into right and left and upper and lower regions, defined when the patient is looking straight ahead. Each eye has its own visual field or, in other words, the part of the world seen by each eye alone. The lateral visual field of an eye is called the temporal field, whereas the medial visual field of the same eye is called the nasal field. Although the fields of vision of the two eyes overlap greatly, the right eye sees things far to the right that the left eye cannot see, and vice versa.
- Optic chiasm. Each optic nerve carries axons from the entire retina of the eye. However, after coursing through their respective optic canals, the right and left optic nerves engage in a redistribution of axons at the optic chiasma, located just anterior to the pituitary stalk. The optic chiasma is created by neurons from the nasal half of each retina crossing over to the opposite side.
- Optic tracts. The two optic tracts emerge from the optic chiasma. The right optic tract contains axons from the temporal half of the right retina and the nasal half of the left retina and carries information about the entire left visual field. The left optic tract contains neurons from the temporal half of the left retina and the nasal half of the right retina and carries information about the entire right visual field. An optic tract is named according to the side of the body on which it lies, but it is concerned with the contralateral visual field.
Injury to CN II may result in monocular blindness. If an optic tract is injured, the result is hemianopia; that is, half the visual field of each eye is lost. Specifically, the half-field of one eye that is lost is the same side as the half-field that is lost by the other eye. The lost fields will be contralateral to the damaged optic tract. For example, interruption of the function in the left optic tract causes loss of vision in the right visual fields of both eyes. In addition, injury to CN II may result in a loss of the papillary reflex of CN III.
Most cranial nerves are peripheral nerves and therefore myelinated by Schwann cells. However, CN II is an extension of the forebrain and as such is myelinated by oligodendrocytes. Multiple sclerosis is an autoimmune disorder that attacks myelin in oligodendrocytes. Therefore, CN II is the only cranial nerve affected by multiple sclerosis.
Eighty percent of the optic nerve consists of visual fibers that synapse in the lateral geniculate body on neurons whose axons terminate in the primary visual cortex of the occipital lobes. Twenty percent of the fibers are pupillary and bypass the geniculate body en route to the pretectal area. Since the ganglion cells of the retina and their axons are part of the central nervous system, they will not regenerate if severed.
Sheaths of the Optic Nerve (Figure 1–25)
The fibrous wrappings that ensheathe the optic nerve are continuous with the meninges. The pia mater is loosely attached to the nerve near the chiasm and only for a short distance within the cranium, but it is closely attached around most of the intracanalicular and all of the intraorbital portions. The pia consists of some fibrous tissue with numerous small blood vessels (Figure 1–26). It divides the nerve fibers into bundles by sending numerous septa into the nerve substance. The pia continues to the sclera, with a few fibers running into the choroid and lamina cribrosa.
|

|

The arachnoid comes in contact with the optic nerve at the intracranial end of the optic canal and accompanies the nerve to the globe, where it ends in the sclera and overlying dura. This sheath is a diaphanous connective tissue membrane with many septate connections with the pia mater, which it closely resembles. It is more intimately associated with pia than with dura.
The dura mater lining the inner surface of the cranial vault comes in contact with the optic nerve as it leaves the optic canal. As the nerve enters the orbit from the optic canal, the dura splits, one layer (the periorbita) lining the orbital cavity and the other forming the outer dural covering of the optic nerve. The dura becomes continuous with the outer two-thirds of the sclera. The dura consists of tough, fibrous, relatively avascular tissue lined by endothelium on the inner surface.
The subdural space is between the dura and the arachnoid; the subarachnoid space is between the pia and the arachnoid. Both are more potential than actual spaces under normal conditions but are direct continuations of their corresponding intracranial spaces. Increased cerebrospinal fluid pressure results in dilatation of the subarachnoid component of the optic nerve sheaths. The meningeal layers are adherent to each other and to the optic nerve and the surrounding bone within the optic foramen, making the optic nerve resistant to traction from either end.
Blood Supply (Figure 1–26)
The surface layer of the optic disk receives blood from branches of the retinal arterioles. In the region of the lamina cribrosa, comprising the prelaminar, laminar, and retrolaminar segments of the optic nerve, the arterial supply is from the short posterior ciliary arteries. The anterior intraorbital optic nerve receives some blood from branches of the central retinal artery. The remainder of the intraorbital nerve, as well as the intracanalicular and intracranial portions, are supplied by a pial network of vessels derived from the various branches of the ophthalmic artery and other branches of the internal carotid.
The Optic Chiasm
The optic chiasm is located at the junction of the floor and anterior wall (lamina terminalis) of the third ventricle. It is variably situated near the top of the diaphragm of the sella turcica, most often posteriorly, lying 1 cm above it and continuing the 45° upward angulation of the optic nerves after their emergence from the optic canals (Figure 1–27). The internal carotid arteries lie just laterally, adjacent to the cavernous sinuses. The chiasm is made up of the junction of the two optic nerves and provides for crossing of the nasal fibers to the opposite optic tract and passage of temporal fibers to the ipsilateral optic tract. The macular fibers are arranged similarly to the rest of the fibers except that their decussation is farther posteriorly and superiorly. The chiasm receives many small blood vessels from the neighboring circle of Willis.
The Retrochiasmatic Visual Pathways
Each optic tract begins at the posterolateral angle of the chiasm and sweeps around the upper part of the cerebral peduncle to end in the lateral geniculate nucleus. Afferent pupillary fibers leave the tract just anterior to the nucleus and pass via the brachium of the superior colliculus to the midbrain. (The pupillary pathway is diagrammed in Figure 14–2.) Afferent visual fibers terminate on cells in the lateral geniculate nucleus that give rise to the geniculocalcarine tract. This tract traverses the posterior limb of the internal capsule and then fans out into a broad bundle called the optic radiation. The fibers in this bundle curve backward around the anterior aspect of the temporal horn of the lateral ventricle and then medially to reach the calcarine cortex of the occipital lobe, where they terminate. The most inferior fibers, which carry projections from the superior aspect of the contralateral half of the visual field, course anteriorly into the temporal lobe in a configuration known as Meyer's loop. Lesions of the temporal lobe that extend 5 cm back from the anterior tip involve these fibers and can produce superior quadrantanopic field defects.
The primary visual cortex (area V1) occupies the upper and lower lips and the depths of the calcarine fissure on the medial aspect of the occipital lobe. Each lobe receives input from the two ipsilateral half-retinas, representing the contralateral half of the binocular visual field. Projection of the visual field onto the visual cortex occurs in a precise retinotopic pattern. The macula is represented at the medial posterior pole, and the peripheral parts of the retina project to the most anterior part of the calcarine cortex. On either side of area V1 lies area V2, and then area V3. V2 appears to function in a manner very similar to V1. Area V4, situated on the medial surface of the cerebral hemisphere but more anterior and inferior than V1 in the region of the fusiform gyrus, is primarily concerned with color processing. Motion detection localizes to area V5 at the junction of the occipital and temporal lobes, lateral to area V1.
The trigeminal nerve is the principal general sensory supply to the head.

A. General sensory innervation from the trigeminal nerve (CN V). B. General sensory distribution of CN V. C. Branchial motor distribution of the mandibular division of the trigeminal nerve (CN V-3) to muscles of mastication.
Pathways
CN V originates from the lateral surface of the pons as a large sensory root and a smaller motor root. These roots enter the trigeminal (Meckel's) cave of the dura, lateral to the body of the sphenoid bone and the cavernous sinus. The sensory root leads to the trigeminal (semilunar) ganglion, which houses the cell bodies for the general sensory neurons. The motor root runs parallel to the sensory root, bypassing the ganglion and becoming part of the mandibular nerve (CN V-3). As well as being the primary general sensory distribution to the head, CN V also aids in distributing postganglionic parasympathetic neurons of the head to their destinations for CNN III, VII, and IX. The trigeminal ganglion gives rise to three divisions, named for the cranial location to the eyes (ophthalmic), the maxilla (maxillary), and the mandible (mandibular).
CN V-1: Ophthalmic Division
CN V-1 courses along the lateral wall of the cavernous sinus and enters the orbit via the superior orbital fissure. CN V-1 provides general sensory innervation to the orbit, cornea, and the skin of the bridge of the nose, scalp and forehead (above the lateral corners of the eye).
 Injury to branches of CN V-1 can result in a loss of sensation in the skin of the forehead and scalp. CN V-1 also innervates the cornea; therefore, mediation of the sensory limb of the corneal reflex is via the nasociliary branch.
Injury to branches of CN V-1 can result in a loss of sensation in the skin of the forehead and scalp. CN V-1 also innervates the cornea; therefore, mediation of the sensory limb of the corneal reflex is via the nasociliary branch.
CN V-2: Maxillary Division
CN V-2 passes through the lateral wall of the cavernous sinus and through the foramen rotundum into the pterygopalatine fossa. This nerve provides general sensory innervation to the maxillary face (between the lateral corners of the eye and the corners of the mouth), including the palate, nasal cavity, paranasal sinuses, and the maxillary teeth.
Injury to branches of CN V-2 can result in a loss of sensation in the skin over the maxilla and maxillary teeth.
CN V-3 courses through the foramen ovale into the infratemporal fossa (Figure 17-4A–C). CN V-3 provides general sensory innervation to the lower part of the face (below the lateral corners of the mouth), including the anterior two-thirds of the tongue, the mandibular teeth, the mandibular face, and even part of the scalp. CN V-3 also has branchial motor neurons, which innervate muscles derived from the first branchial arch which include the muscles of mastication (temporalis, masseter, and medial and lateral pterygoid muscles), mylohyoid, anterior belly of the digastricus, tensor tympani, and tensor veli palatine muscles.
Injury to branches of CN V-3 can result in a loss of sensation in the mandibular skin and teeth as well as the anterior two-thirds of the tongue. Because the motor division of CN V-3 innervates the muscles of mastication (e.g., temporalis and masseter muscles), the patient may experience weakness in chewing and deviation of the mandible on the side of the lesion when the mouth is opened.
The Trigeminal Nerve (V) (Figure 1–3)
The trigeminal nerve originates from the pons, and its sensory roots form the trigeminal ganglion. The first (ophthalmic) of the three divisions passes through the lateral wall of the cavernous sinus and divides into the lacrimal, frontal, and nasociliary nerves. The lacrimal nerve passes through the upper lateral aspect of the superior orbital fissure, outside the annulus of Zinn, and continues its lateral course in the orbit to terminate in the lacrimal gland, providing its sensory innervation. Slightly medial to the lacrimal nerve within the superior orbital fissure is the frontal nerve, which is the largest of the first division of branches of the trigeminal nerve. It also crosses over the annulus of Zinn and follows a course over the levator to the medial aspect of the orbit, where it divides into the supraorbital and supratrochlear nerves. These provide sensation to the brow and forehead. The nasociliary nerve is the sensory nerve of the eye. After entering through the medial portion of the annulus of Zinn, it lies between the superior rectus and the optic nerve. Branches to the ciliary ganglion and those forming the ciliary nerves provide sensory supply to the cornea, iris, and ciliary body. The terminal branches are the infratrochlear nerve, which supplies the medial portion of the conjunctiva and eyelids, and the anterior ethmoidal nerve, which provides sensation to the tip of the nose. Thus, the skin on the tip of the nose may be affected with vesicular lesions prior to the onset of herpes zoster ophthalmicus.
The second (maxillary) division of the trigeminal nerve passes through the foramen rotundum and enters the orbit through the inferior orbital fissure. It passes through the infraorbital canal, becoming the infraorbital nerve, and exits via the infraorbital foramen, supplying sensation to the lower lid and adjacent cheek. It is frequently damaged in fractures of the orbital floor.
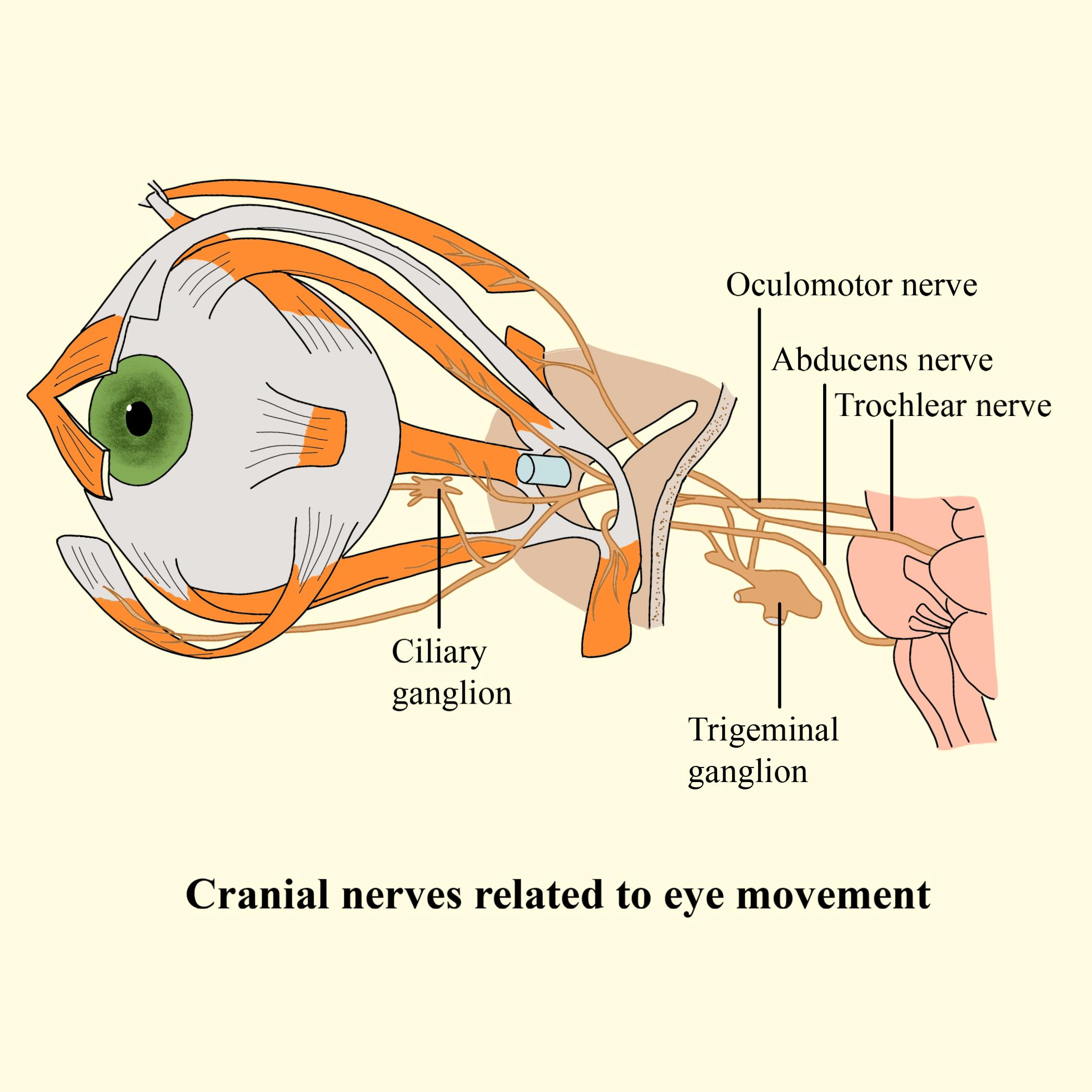
The abducens nerve innervates the lateral rectus muscle.
Pathways
The abducens nerve originates from the pons and courses through the cavernous sinus, entering the orbit via the superior orbital fissure (Figure 17-3A). The abducens nerve supplies somatic motor innervation to the lateral rectus muscle, which abducts the eye.
Injury to CN VI, the cavernous sinus, or the orbit may result in the inability to move the eye laterally, resulting in diplopia on lateral gaze.
The Oculomotor Nerve (III)
The oculomotor nerve leaves the brainstem between the cerebral peduncles and passes near the posterior communicating artery of the circle of Willis. Lateral to the pituitary gland, it is closely approximated to the optic tract, and here it pierces the dura to course in the lateral wall of the cavernous sinus. As the nerve leaves the cavernous sinus, it divides into superior and inferior divisions. The superior division enters the orbit within the annulus of Zinn at its highest point and adjacent to the trochlear nerve (Figure 1–3). The inferior division enters the annulus of Zinn low and passes below the optic nerve to supply the medial and inferior rectus muscles. A large branch from the inferior division extends forward to supply the inferior oblique. A small twig from the proximal end of the nerve to the inferior oblique carries parasympathetic fibers to the ciliary ganglion.
The Abducens Nerve (VI)
The abducens nerve (Figure 1–3) originates between the pons and medulla and pursues an extended course, having the longest intracranial course of any cranial nerve, up the clivus to the posterior clinoid, penetrates the dura, and passes within the cavernous sinus. (All other nerves course through the lateral wall of the cavernous sinus.) After passing through the superior orbital fissure within the annulus of Zinn, the nerve continues laterally to innervate the lateral rectus muscle.
The facial nerve provides motor innervation to the muscles of facial expression, lacrimal gland, and submandibular and sublingual salivary glands, as well as taste to the anterior two-thirds of the tongue.
The facial nerve is one of the 12 cranial nerves that emerge directly from the brain. Marked as cranial nerve 7 (VII), the facial nerve exits the brain, giving off branches along its way to the parotid gland where it divides into five smaller nerves.
The facial nerve is responsible for motor, sensory and parasympathetic functions of structures in the head.

Motor
- Facial muscles
- Stapedius muscle
Sensory
- Anterior two-thirds of the tongue
Parasympathetic
- Salivary and lachrymal glands
CN VII Modalities
The facial nerve traverses the internal acoustic meatus carrying four modalities.
- Branchial motor neurons. Supply muscles derived from the second branchial arch including the muscles of facial expression as well as the stapedius, posterior belly of the digastricus, and stylohyoid muscles.
- Visceral motor neurons. Provide parasympathetic innervation to almost all glands of the head (e.g., lacrimal, submandibular, sublingual, nasal, and palatal). The only exception is the parotid gland, which receives its visceral motor innervation from CN IX.
- Special sensory neurons. Transmit taste sensation from the anterior two-thirds of the tongue.
- General sensory neurons. Transmit general sensation from a portion of the external acoustic meatus and auricle.

A. The facial nerve (CN VII). B. Branchial motor innervation for CN VII. C. Special sensory distribution of the vestibulocochlear nerve (CN VIII).
CN VII Branches
Two distinct fascial sheaths package the four modalities carried by CN VII, with branchial motor neurons in one sheath and visceral motor, special sensory, and general sensory neurons in another sheath called the nervus intermedius.
Branchial Motor Nerve Trunk
The branchial motor components constitute the largest portion of CN VII. After entering the temporal bone via the internal acoustic meatus, a small branch of CN VII courses to the stapedius muscle, where branchial motor neurons course through the facial canal to exit the skull via the stylomastoid foramen. In the parotid gland, five terminal branches (i.e., temporal, zygomatic, buccal, mandibular, and cervical) provide voluntary control of the muscles of facial expression, including the buccinator, occipitalis, platysma, posterior digastricus, and stylohyoid muscles.
Nervus Intermedius
The nervus intermedius gives rise to the following nerves:
- Greater petrosal nerve. Contains preganglionic parasympathetic neurons that synapse in the pterygopalatine ganglion en route to the lacrimal, nasal, and palatine glands.
- Chorda tympani. Arises in the descending part of the facial canal and crosses the medial aspect of the tympanic membrane, passing between the malleus and incus. The chorda tympani exits the skull through the petrotympanic fissure and joins the lingual nerve from CN V-3 in the infratemporal fossa. The chorda tympani contains preganglionic parasympathetic neurons that synapse in the submandibular ganglion en route to innervate the submandibular and the sublingual salivary glands. The chorda tympani also contains special sensory neurons (taste) from the anterior two-thirds of the tongue, with cell bodies located in the geniculate ganglion.
- Auricular branches. Arise from the external acoustic meatus and auricle and carry general sensory neurons through the geniculate ganglion to the brainstem. The geniculate ganglion is a knee-shaped bend in CN VII, located within the temporal bone and housing sensory cell bodies for the special sensory neurons for taste and general sensory neurons from the ear.
Injury to CN VII, after it exits the brainstem, results in paralysis of the facial muscles (Bell's palsy) on the ipsilateral side. Fracture of the temporal bone can result in the abnormalities just described, plus increased sensitivity to noise (hyperacusis) due to the lack of innervation to the stapedius muscle, dry mouth due to a decrease in salivation, dry corneas due to the lack of lacrimal gland activity, and a loss of taste on the anterior two-thirds of the tongue. It should be noted that a brainstem injury to CN VII results in paralysis of the contralateral facial muscles below the eye.
The Facial Nerve (VII)
The facial nerve exits the brainstem at the lower border of the pons, the greater petrosal nerve forming part of the separate portion known as the nervus intermeidus, and passes through the internal acoustic meatus with the vestibulocochlear (VII) nerve into the facial canal. At the geniculate ganglion the greater petrosal nerve, which contains parasympathetic secretomotor fibers, joins the lesser petrosal nerve to form the nerve of the pterygoid canal (Vidian nerve) and pass through the pterygopalatine ganglion, where the parasympathetic fibers synapse, to reach the lacrimal gland. The facial nerve exits the facial canal at the stylomastoid foramen, passes through the parotid gland and then branches out across the face to supply the muscles of facial expression, including orbicularis oculi.
CN VIII: Vestibulocochlear Nerve
The vestibulocochlear nerve traverses the internal acoustic meatus with CN VII and has the following modalities (Figure 17-5B):
- Special sensory neurons. CN VIII originates from the grooves between the pons and the medulla oblongata. CN VIII divides into the cochlear branch to the cochlea (hearing) and the vestibular branch to the semicircular canal (equilibrium).
Injury to CN VIII can result in ipsilateral deafness, tinnitus (ringing in the ear), and vertigo (loss of balance).
The glossopharyngeal nerve provides motor innervation to the stylopharyngeus muscle and parotid gland and sensory innervation from the carotid body and sinus, posterior one-third of the tongue, and the auditory tube.
The glossopharyngeal nerve emerges from the lateral aspect of the medulla oblongata and traverses the jugular foramen, where its superior and inferior sensory ganglia are located (Figure 17-6).

The glossopharyngeal nerve (CN IX).
Modalities
CN IX consists of the five modalities described as follows.
- Branchial motor neurons. Course in a pharyngeal branch to innervate the stylopharyngeus muscle the only skeletal muscle derived from the third branchial arch. CN IX then courses between the superior and middle pharyngeal constrictor muscles en route to the oropharynx and the tongue.
- Visceral motor neurons. Parasympathetic neurons from CN IX innervate the parotid gland via the following pathway:
- Preganglionic parasympathetic neurons originate in the inferior salivatory nucleus and enter the petrous part of the temporal bone via the tympanic canaliculus to the tympanic cavity.
- Within the tympanic cavity, the tympanic nerve forms the tympanic plexus on the promontory of the middle ear to provide general sensation to the tympanic membrane and nearby structures. The visceral motor preganglionic parasympathetic neurons course through the plexus and merge to become the lesser petrosal nerve.
- The lesser petrosal nerve reenters and travels through the temporal bone to emerge in the middle cranial fossa, lateral to the greater petrosal nerve. The lesser petrosal nerve then proceeds anteriorly to exit the skull via the foramen ovale with CN V-3.
- Upon exiting the skull, preganglionic parasympathetic neurons within the lesser petrosal nerve synapse in the otic ganglion. Postganglionic parasympathetic neurons exit the otic ganglion and travel with the auriculotemporal branch of CN V-3 to innervate the parotid gland.
- General sensory neurons. Course within the tympanic plexus, providing innervation to the internal surface of the tympanic membrane, the middle ear, and the auditory tube. General sensory neurons also course in the pharyngeal branch from the posterior third of the tongue and the oropharynx.
- Special sensory neurons. Course from the posterior third of the tongue within the pharyngeal branch of CN IX, providing taste sensation to the brain.
- Visceral sensory neurons. Course from the carotid sinus and carotid body and ascend in the sinus nerve, joining CN IX. The cell bodies of the visceral sensory neurons reside in the inferior ganglion.
Injury to CN IX may result in loss of the gag reflex, alteration in taste to the posterior third of the tongue, and altered vasovagal reflex.
The vagus nerve innervates muscles of the larynx, pharynx, palate in addition to the gut tube, heart and lungs.
The vagus nerve emerges from the lateral aspect of the medulla oblongata and traverses the jugular foramen, where the superior and inferior sensory ganglia are located.
The vagus nerve exits the medulla oblongata and travels with CNN IX and XI into the jugular foramen. CN X consists primarily of the following four modalities:
- Visceral sensory neurons. Provide visceral sensory information from the larynx (below the vocal folds), trachea, and esophagus, and the thoracic and abdominal viscera as well as the stretch receptors of the aortic arch and the chemoreceptors of the aortic and carotid bodies (Figure 17-7A and B).
- General sensory neurons. Provide general sensory information from part of the external acoustic meatus, the pinna, and the laryngopharynx (Figure 17-7A).
- Branchial motor neurons. Supply the palatoglossus, laryngeal, and pharyngeal muscles (except for the stylopharyngeus muscle, which is supplied by CN IX) and the palatal muscles (except for the tensor veli palatini, which is supplied by CN V-3) (Figure 17-7A).
- Visceral motor neurons. Provide parasympathetic innervation to the smooth muscle and the glands of the respiratory system and gastrointestinal tract to the transverse colon (Figure 17-7B). In general, CN X increases secretion from glands and smooth muscle contraction. CN X slows the heart rate, stimulates bronchiolar secretions, bronchoconstriction, and peristalsis, and increases secretions.

Distribution of the vagus nerve (CN X) to the head and neck (A) and the thorax and abdomen (B).
Upon traversing the jugular foramen, CN X travels between the internal jugular vein and the internal carotid artery within the carotid sheath.
The branchial motor fibers exit the vagus nerve as the following branches:
- Pharyngeal branch. The pharyngeal branch is the principal motor innervation of the pharyngeal muscles. It branches just below the inferior vagal ganglion and courses between the internal and external carotid arteries. The pharyngeal branch then enters the middle pharyngeal constrictor muscle, where it forms the pharyngeal plexus. The pharyngeal plexus innervates all of the pharyngeal muscles (i.e., superior, middle, and inferior pharyngeal constrictors; salpingopharyngeus, palatopharyngeus, palatoglossus, and levator veli palatini), with the exception of the stylopharyngeus muscle by CN IX and the tensor veli palatini by CN V-3.
- Superior laryngeal branch. The superior laryngeal nerve branches immediately below the pharyngeal nerve. The nerve descends in the neck adjacent to the pharynx and splits to form the following nerves:
- External laryngeal nerve. Provides branchial motor innervation to part of the inferior pharyngeal constrictor muscle and the cricothyroideus muscle.
- Internal laryngeal nerve. Pierces the thyrohyoid membrane and provides general sensory innervation of the larynx above the vocal folds.
- Recurrent laryngeal branch. The path of the recurrent laryngeal nerve differs on the right and left sides of the body.
- Left recurrent laryngeal nerve. Branches from the vagus nerve at the level of the aortic arch. The nerve loops posteriorly around the aortic arch by the ligamentum arteriosus and ascends through the superior mediastinum to enter the groove between the esophagus and the trachea.
- Right recurrent laryngeal nerve. Branches from the vagus nerve before entering the superior mediastinum at the level of the right subclavian artery. The nerve hooks posteriorly around the subclavian artery and also ascends in the groove between the esophagus and trachea.
- Both recurrent laryngeal nerves pass deep to the lower margin of the inferior constrictor muscle to innervate the intrinsic laryngeal muscles and visceral sensory innervation below the vocal folds.
Injury to CN X may result in hoarseness (due to paralysis of the intrinsic laryngeal muscles) and difficulty swallowing (due to paralysis of pharyngeal muscles). On examination, the soft palate droops on the affected side, and the uvula deviates opposite the affected side as a result of the unopposed action of the intact levator veli palatini muscle. There also may be loss of the gag reflex, where CN IX provides the sensory limb and CN XI provides the motor limb through innervation of the pharyngeal muscles.
The spinal accessory nerve originates from the medulla oblongata, exits the jugular foramen, and provides branchial motor innervation to the trapezius and sternocleidomastoid muscles (Figure 17-8).

The spinal accessory nerve (CN XI) and the hypoglossal nerve (CN XII).
Injury to CN XI may result in weakness in turning the head to the opposite side and in shoulder drop.
The hypoglossal nerve exits the medulla oblongata in the groove between the pyramid and the olive (Figure 17-8). Upon exiting the hypoglossal canal, CN XII courses between the internal carotid artery and the internal jugular vein, deep to the posterior digastricus muscle. CN XII then courses along the lateral surface of the hyoglossus muscle deep to the mylohyoid muscle. CN XII provides somatic motor innervation to all intrinsic and extrinsic tongue muscles (with the exception of the palatoglossus, supplied by CN X).
 Injury to CN XII can be assessed by having the patient stick the tongue straight out. If there is a lesion on CN XII, the tongue will protrude toward the affected side. A way to remember this is that a patient with a lesion of CN XII will “lick his wound.”
Injury to CN XII can be assessed by having the patient stick the tongue straight out. If there is a lesion on CN XII, the tongue will protrude toward the affected side. A way to remember this is that a patient with a lesion of CN XII will “lick his wound.”
All preganglionic sympathetic neurons destined for the head originate at the T1 level of the spinal cord and synapse in the superior cervical ganglion. Postganglionic sympathetic neurons course along cranial arteries to the end organs such as the sweat glands, the superior tarsal muscle, and the dilator pupillae muscle.
Preganglionic parasympathetic neurons originate in the brainstem, course in CNN III, VII, IX, or X, and synapse in one of four ganglia (i.e., ciliary, pterygopalatine, submandibular, and otic). Postganglionic parasympathetic neurons then course along nerves to their end organs (e.g., salivary glands and pupillary sphincter muscle).
Sympathetic Innervation
Remember that all preganglionic sympathetic neurons in the body originate at spinal cord levels T1–L2 (Figure 17-9). Therefore, all visceral motor sympathetic innervation to the head originates in the upper levels of the thoracic spinal cord, with most originating at the T1 level.
- Preganglionic sympathetic fibers. Originate from T1 of the spinal cord, ascend in the sympathetic trunk, and synapse with postganglionic fibers in the superior cervical ganglion.
- Postganglionic sympathetic fibers. Originate in the superior cervical ganglion and follow the arteries throughout the head to innervate the blood vessels, sweat glands, superior tarsal muscle (to elevate the upper eyelid), and the dilatator pupillae muscle (to dilate the pupil).
-

Autonomic innervation of the head.
Lesions in the sympathetic neurons to the head result in Horner's syndrome. Patients with Horner's syndrome usually present with ptosis (eyelid droop), miosis (constricted pupil), anhydrosis (loss of sweating), and flushed face.
There are four parasympathetic ganglia associated with the cranial nerves (Figure 17-9; Table 17-3).
- Ciliary ganglion. Located posterior to the eyeball between the optic nerve and the lateral rectus muscle. Preganglionic parasympathetic neurons from the inferior division of CN III synapse in the ciliary ganglion and send postganglionic parasympathetic neurons to the sphincter pupillae and the ciliary muscles via the short ciliary nerves.
- Pterygopalatine ganglion. Located in the pterygopalatine fossa, just inferior to CN V-2 and lateral to the sphenopalatine foramen. Preganglionic parasympathetic neurons from CN VII synapse in the pterygopalatine ganglion and send postganglionic parasympathetic neurons to the lacrimal, nasal, and palatal glands.
- Submandibular ganglion. Suspended from the lingual nerve of CN V-3, deep to the mylohyoid muscle. Preganglionic parasympathetic neurons from CN VII synapse in the submandibular ganglion and send postganglionic parasympathetic neurons to supply the submandibular and sublingual salivary glands.
- Otic ganglion. Located in the infratemporal fossa inferior to the foramen ovale between CN V-3 and the tensor veli palatini muscle. Preganglionic parasympathetic neurons from CN IX synapse in the otic ganglion and send postganglionic neurons in the auriculotemporal nerve of CN V-3 to supply the parotid gland.
- Table 17-3. Parasympathetic Innervation of the Head
CN
Preganglionic Parasympathetic Cell Body Origin
Postganglionic Parasympathetic Cell Body Origin
Function
CN III (oculomotor)
Edinger–Westphal nucleus
Ciliary ganglion
Sphincter pupillae m. (constricts pupil) and ciliary m. (lens accommodation for near vision)
CN VII (facial)
Superior salivatory nucleus
Pterygopalatine ganglion
Submandibular ganglion
Lacrimal, nasal, and palatal glands
Submandibular and sublingual salivary glands
CN IX (glossopharyngeal)
Inferior salivatory nucleus
Otic ganglion
Parotid gland
CN X (vagus)
Posterior vagal nucleus
Intramural ganglia
Innervates heart, smooth muscle of respiratory tract, gastrointestinal tract (up to splenic flexor), and viscera associated with foregut and midgut
There are four cranial nerves that carry visceral motor parasympathetic innervation to the head: CNN III, VII, IX, and X.
- CN III (oculomotor nerve). Preganglionic parasympathetic neurons synapse in the ciliary ganglion, with postganglionic parasympathetic neurons serving the ciliary muscles and sphincter pupillae for light accommodation and constriction of the pupil.
- CN VII (facial nerve). Preganglionic neurons traveling in the greater petrosal nerve synapse in the pterygopalatine ganglion, with postganglionic parasympathetic neurons coursing to serve the lacrimal, nasal, and palatal glands. Preganglionic neurons from CN VII also travel within the chorda tympani nerve to synapse in the submandibular ganglion, with postganglionic neurons serving the submandibular and sublingual salivary glands.
- CN IX (glossopharyngeal nerve). Preganglionic parasympathetic neurons synapse in the otic ganglion, with postganglionic parasympathetic neurons serving the parotid gland.
- CN X (vagus nerve). Preganglionic parasympathetic neurons synapse at or near the target organ, with postganglionic parasympathetic neurons serving smooth muscle and glands of the gastrointestinal tract to the transverse colon.